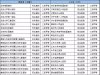
据世界卫生组织(WHO)官网15日报道,由于缺乏诊断设备,目前仍有许多人无法进行疾病检测。为此,该机构发布了全球首份用于指导诊断常见疾病和若干优先处理疾病的基本诊断清单,希望能帮助提高诊断准确率并改善治疗结果。 这份清单主要针对包括血液和尿液等人体标本测试在内的体外测试。它包含113种产品,其中58种用于检测和诊断各种常见病症,为病人筛查和管理奠定了基础;另外55种主要用于检测、诊断和监测艾滋病、结核病、疟疾、乙型和丙型肝炎、人乳头瘤病毒以及梅毒等被世卫组织列为优先处理的疾病。 另据新华社报道称,对于每个类别的测试,基本诊断清单都规定了测试类型和预期用途,以及是否适用于初级卫生保健机构或具有化验室的大型医疗设施。与已使用40年的世卫组织基本药物清单类似,基本诊断清单旨在供各国制定或更新其诊断清单时参考。 世卫组织表示,清单中一些测试特别适用于那些化验室资源有限、甚至根本没有化验室的初级卫生保健机构,比如能够快速诊断儿童急性疟疾的测试,以及用于检测糖尿病的血糖仪等。这些检测不依赖电力,操作人员也无需经过培训。
World Health Organization Model List of Essential In Vitro Diagnostics
First edition (2018)
16 May
2018
Acronyms
|
ALT
|
alanine aminotransferase
|
|
AMR
|
antimicrobial resistance
|
|
AST
|
aspartate aminotransferase
|
|
BMP
|
basic metabolic panel
|
|
BUN
|
blood urea nitrogen
|
|
CBC
|
complete blood count
|
|
CLIA
|
chemiluminescence immunoassay
|
|
CRP
|
C-reactive protein
|
|
CSF
|
cerebrospinal fluid
|
|
CVD
|
cardiovascular disease
|
|
DST
|
drug susceptibility testing
|
|
ECL
|
electrochemiluminescence
|
|
EDL
|
World Health Organization
Model List of Essential In Vitro
Diagnostics
|
|
eGFR
|
estimated glomerular
filtration rate
|
|
EIA
|
enzyme immunoassay
|
|
ELISA
|
enzyme linked immunosorbent
assay
|
|
EML
|
World Health Organization
Model List of Essential
Medicines
|
|
EPTB
|
extrapulmonary tuberculosis
|
|
GPW
|
WHO General Programme of Work
|
|
Hb
|
haemoglobin
|
|
HbA1c
|
haemoglobin A1c
|
|
hCG
|
human chorionic gonadotropin
|
|
Ht
|
haematocrit
|
|
HTLV
|
human T-lymphotropic virus
|
|
IGRA
|
interferon gamma release assay
|
|
INR
|
international normalized ratio
|
|
IVDs
|
in vitro diagnostics
|
|
LAMP
|
loop mediated isothermal
amplification
|
|
LPA
|
line probe assay
|
|
NAT
|
nucleic acid test
|
|
NCDs
|
noncommunicable diseases
|
|
PQ
|
WHO Prequalification
|
|
PT
|
prothrombin time
|
|
RBC
|
red blood cell count
|
|
RDT
|
rapid diagnostic test
|
|
SAGE-IVD
|
Strategic Advisory Group of
Experts on In Vitro Diagnostics
|
|
TB
|
Mycobacterium tuberculosis
|
|
TST
|
tuberculin skin test
|
|
UTI
|
urinary tract infection
|
|
VHF
|
viral haemorrhagic fever
|
|
WBC
|
white blood cell count
|
|
WHO
|
World Health Organization
|
Preface
Introduction
The World Health
Organization (WHO) published the first edition of the Model List of Essential
In Vitro Diagnostics (EDL) in May 2018, in recognition that IVDs are an
essential component to advance universal health coverage, address health
emergencies, and promote healthier populations, which are the three strategic
priorities of the WHO Thirteenth General Programme of Work (2019–2023) (GPW).
The EDL is also intended to complement the WHO Model List of Essential
Medicines (EML) and enhance its impact.
Objectives of the Model
List of Essential In Vitro Diagnostics (EDL)
The EDL outlines a group of
IVDs that are recommended by WHO for use at various levels of a tiered national
health care system. The EDL is not intended to be prescriptive with respect to
the IVDs listed or the levels at which such IVDs can/should be used; rather
country programmes should make the ultimate decisions about which IVDs are
selected and where they are implemented, based on national or regional burden
of disease, unmet needs and priorities.
It is
expected that the EDL will provide guidance and serve as a reference to Member
States (including ministries of health, programme
managers, end users such as laboratory managers, procurement officers and
reimbursement systems), who are developing and/or
updating lists of national essential IVDs for defining universal health
coverage interventions, as well as selecting and implementing such IVDs.
It will also inform United Nations agencies and nongovernmental organizations
that support selection, procurement, supply, donations or provision of IVDs.
Finally, it will inform and guide the medical technology private sector on IVD
priorities and the IVDs needed to address global health issues.
While the EDL provides a
list of important tests required at various levels of the health care system,
it is important to note that the EDL itself cannot have an impact without an
integrated, connected, tiered laboratory system, with adequate human resources,
training, laboratory infrastructure, and regulatory/quality assurance systems.
Impact also requires Member States to adopt and adapt the EDL and develop
national and regional EDLs, as well as to implement the selection and supply
mechanisms necessary to ensure access to the
IVDs.
Scope of the first
edition of the EDL
Based on the EDL
selection criteria described below, the EDL consists:
·
A group of general laboratory
tests that can be used for routine patient care as well as for the detection
and diagnosis of a wide array of disease conditions – communicable and NCDs.
These IVDs are grouped by test discipline (e.g. clinical chemistry, serology,
haematology, microbiology and mycology) and specific test type (e.g. bilirubin,
complete blood count, etc.).
·
IVDs designed for the
detection, diagnosis and monitoring of each of the following WHO key disease
areas: HIV, TB, malaria, HBV/HCV, and HPV and syphilis. These IVDs are grouped
by disease area and analyte tested.
The EDL does not list specific test brands, but
rather consists of IVDs described according to their biological targets. Where
specific products in categories of tests contained in the EDL have been
prequalified by WHO or are recommended by a WHO disease programme, a link is
provided to that information, which is updated regularly.
EDL content and format
For each specific test listed in the first
edition of the EDL, the following are described:
·
Test purpose: Purpose
for which the test can be utilized.
·
Assay format: The assay
format or formats in which the test is generally
available,
e.g. enzyme immunoassay, nucleic acid testing.
·
Specimen type: The
types of specimens that can be used for the
test.
·
Facility level: The
level of the tiered health care delivery system for which the test is
suggested, as described below.
·
Link to WHO guidance: If there is existing WHO
guidance available on the test or
category of testing, a link is provided to the appropriate location
on the WHO website.
·
WHO PQ or endorsed products:
For each specific test for which there are brands of products
either prequalified by WHO or otherwise endorsed by WHO, a link is
provided.
The EDL is presented by health care facility level in
two tiers: I IVDs for Primary health care;
II IVDs for Health care facilities with clinical
laboratories.
Recommended use of the EDL
In order to effectively use
the EDL and adapt it to national needs, WHO recognizes that Member States will
need to consider a variety of factors. These include, among others: local
demographics and burden of disease; local disease elimination priorities; local
availability of treatments; training and experience of available personnel;
local unmet needs and testing gaps; supply chain and transport links; quality
assurance capacity; financial resources; information technology capabilities;
and environmental factors.
To that end, information
that supports the selection and use of IVDs on the EDL, such as relevant WHO
clinical guidelines, selected systematic reviews, key references, lists of
prequalified IVDs and IVDs recommended by WHO disease control departments, as
well as other relevant resources on quality assurance, basic techniques,
procurement and maintenance guidance, will be collated and maintained on the
WHO website on an IVD-specific webpage linked to the EDL.
The EDL should not be used
in isolation, but in the context of the scope of testing services that meet the
clinical needs and expectations in each country through their own particular
laboratory networks. An illustrative example of a tiered health care delivery
and laboratory network in resource-limited countries is set out in Figure 1.
The pyramid of testing reflects that there are generally a large number of
primary care facilities and that they serve most patients directly for primary
care needs. As one goes up the levels of the system, there are a smaller number of
centralized facilities
serving fewer patients directly. In the case of national reference laboratories
and some provincial laboratories, they may not serve patients directly or they
may offer a broad set of specialist consultative services, and act more as
referral centres for quality assurance and training or for conducting complex
tests (either using samples drawn at facilities lower in the system and
transported or by receiving patients referred directly from other facilities).
Figure 1. The types of
testing that are appropriate at each tier will be country-specific and will
include, among others, factors such as access to electricity, reagent grade
water, phlebotomy and specialized human resources.1
For purposes of the first
edition of the EDL and to simplify its presentation and use, IVDs are listed
for two tiers: primary care settings where no or minimal laboratories are available (Level I in Figure
1) or for laboratory-based facilities (Levels II, III, and IV in Figure 1).
Process of development
of the first edition of the EDL
In March 2017, the WHO
Expert Committee on Selection and Use of Essential Medicines recommended that
an EDL be developed. In support of that recommendation, WHO created an EDL
Secretariat, which drafted the first edition of the EDL in consultation with colleagues
in the various WHO disease programmes. It was then posted online for open
consultation. WHO also created a Strategic Advisory Group of Experts on In
Vitro Diagnostics (SAGE-IVD) to support the development of the EDL and to
advise on other IVD policies and initiatives. SAGE-IVD held its first meeting
from 16–20 April 2018 at WHO headquarters, Geneva, where it made
recommendations for the content, format and implementation of the first edition
of the EDL, as well as its processes moving
forward.
Selection of IVDs for inclusion in the first edition of
the EDL
The selection of the diagnostics tests for
the EDL took into account the following priorities:
| 

 /3
/3 

 浙公网安备33010802005999号
浙公网安备33010802005999号